
V940/mRNA-4157 at 5 Years: Personalized mRNA Oncology Survives the Durability Test
The science is maturing. The real bottleneck is still personalized manufacturing.
The Signal
Jan 20, 2026 — Merck (with Moderna) announced 5-year follow-up data from KEYNOTE-942/mRNA-4157-P201 in high-risk melanoma: the personalized mRNA neoantigen therapy (intismeran autogene) plus pembrolizumab showed sustained improvement in recurrence-free survival vs pembrolizumab alone. A related Cancer Discovery news item also highlighted durable benefit at 5 years.
RapidGene Take
If this holds in Phase 3, it doesn’t just validate one asset—it validates a new industrial stack: tumor sequencing → neoantigen selection → individualized GMP batch → on-time release. That is not a drug; it’s a supply chain. The uncomfortable truth: personalized mRNA oncology will never scale like a vialed vaccine unless the industry makes peace with what it is—software + manufacturing automation + ruthless turnaround discipline. The clinical signal is real; the commercial question is whether you can deliver it fast enough, cheaply enough, and consistently enough to fit into oncology workflows without collapsing under QC/release complexity.
Expanded Read
What this therapy actually is
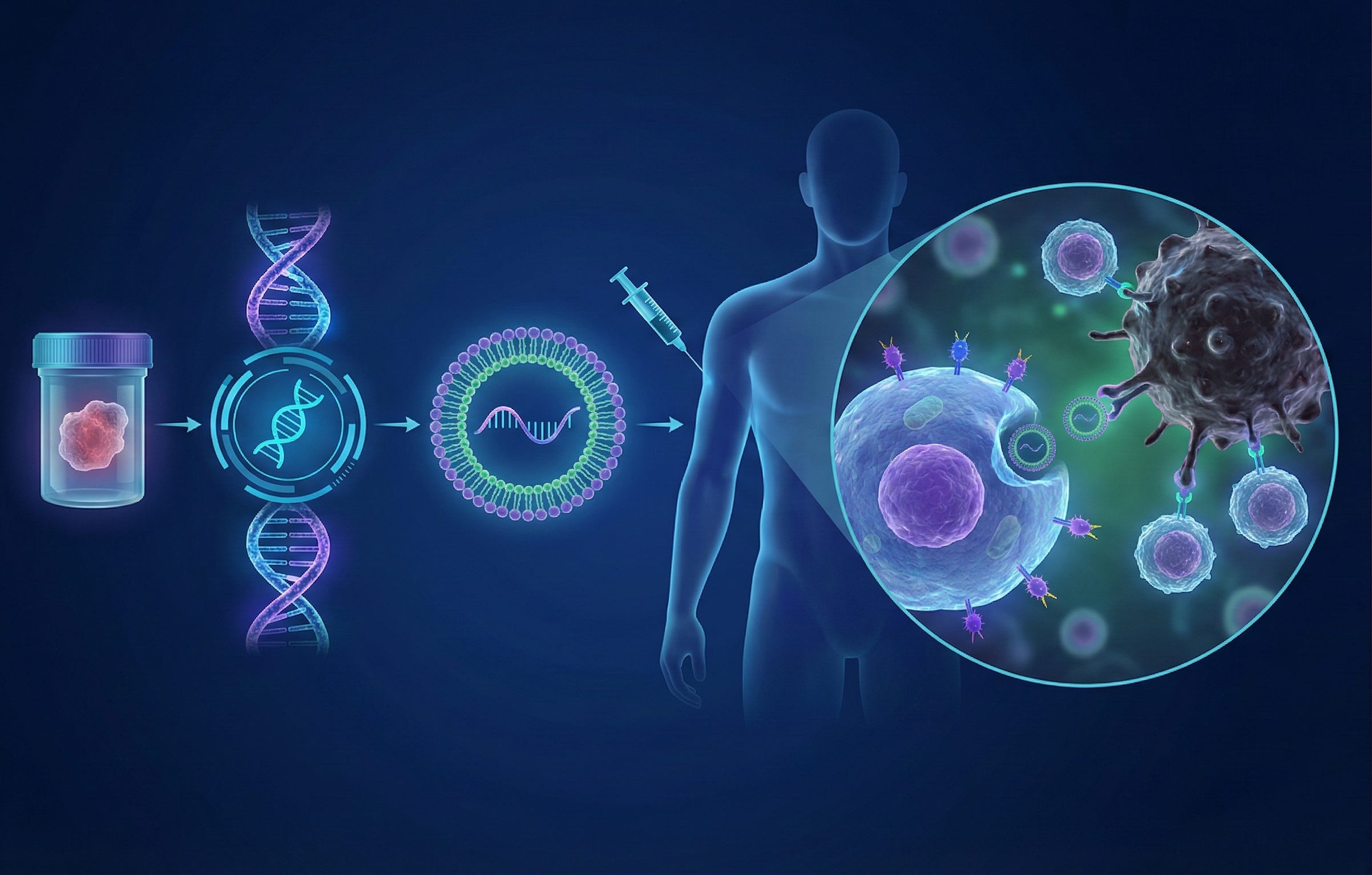
mRNA-4157/V940 is an individualized neoantigen therapy: tumor tissue is sequenced, neoantigens are algorithmically selected, and the resulting sequences are encoded into mRNA so the patient’s cells express neoantigen peptides that prime T-cell responses. Merck’s own description emphasizes endogenous translation and antigen processing/presentation as the bridge to adaptive immunity.
Trial basics (from Merck’s disclosure)
KEYNOTE-942 is a randomized, open-label Phase 2b trial (157 patients) in resected high-risk stage III/IV melanoma. Patients received the individualized therapy 1 mg every three weeks for nine doses plus pembrolizumab (up to ~1 year), vs pembrolizumab alone. Primary endpoint: recurrence-free survival; secondary endpoints include distant metastasis-free survival and safety.
Why 5-year durability is a meaningful signal
Immuno-oncology is littered with early curves that converge. Durable separation at multi-year follow-up suggests real immunologic memory and/or sustained tumor control—particularly relevant when the mechanism is neoantigen-specific T-cell priming.
The “hidden” technical differentiator: not mRNA, but workflow integration
Personalized vaccines are constrained by:
turnaround time (sequencing → design → manufacture)
chain-of-identity and chain-of-custody
individualized release testing strategy (what’s the “identity” test when every batch is unique?)
comparability and process validation in a product that changes every patient.
This is why success here translates into a competitive advantage for whoever operationalizes it: it rewards automation, digital QC, and tightly controlled manufacturing templates more than clever immunology marketing.
CMC reality (the part investors forget, but regulators don’t)
Individualized products must demonstrate:
robust platform controls (same process, different sequence)
impurity controls (dsRNA, truncations, residuals)
potency/translation proxies that scale across sequences
stability and shipping integrity compatible with oncology clinic operations.
If Phase 3 works, regulatory conversations won’t be “does mRNA work?” They’ll be “can you consistently manufacture thousands of individualized lots with acceptable deviation rates?”
Keywords: personalized cancer vaccine, neoantigen mRNA, oncology manufacturing
Disclaimer: RapidGene Insights provides technical and strategic opinions based on public data. This is not investment advice. If you believe our comments lack context, please contact us.
Sources: Merck press release (trial design + regimen); Cancer Discovery news entry via PubMed.